

Thyro-bolic-pause
Have you ever considered that the symptoms of perimenopause mimic that of hypothyroidism or metabolic syndrome (insulin resistance):- weight gain, high cholesterol, heavy and irregular periods, fatigue, insomnia, drying skin and hair, hair loss - enter THYRO-BOLIC-PAUSE.
We know all hormones dance together and impact physiology, some key interactions with these conditions:
➡️ Both thyroid disease & perimenopause increase risk of insulin resistance and a loss of metabolic flexibility (being able to switch from burning sugar to fat)
➡️ Insulin resistance exacerbates perimenopause symptoms
➡️ Perimenopause provides a window of immune dysregulation and autoimmune thyroid disease
Let's start with perimenopause. The time of Perimenopause, from our late 30’s - late 40’s is likened to our 2nd puberty as it relates to a period of significant hormonal changes. Progesterone levels drop dramatically, leaving oestrogen levels unopposed and erratic. Dropping progesterone reduces free or available thyroid

The remaining unopposed and fluctuating oestrogen in perimenopause increases the level of thyroid-binding globulin which as the name might suggest binds up thyroid hormone which means less available thyroid hormone and can be part of the trigger cascade of autoimmunity that underlies most cases of underactive thyroid.
Your symptoms may very well be hypothyroidism, or your peri symptoms can be exacerbated by low functioning thyroid. “We'' need to work across the entire web to ensure the correct “treatment” is provided. To be 100% clear hormone replacement therapy (HRT or Levothyroxine) will not be the magic bullet if other aspects on the web are still present - symptoms will persist.
The concept of Thyro-Bolic Pause, is when any number of hormones can be contributing to an array of symptoms. As to the efficiency of these hormones and operating systems, multiple factors, from missing nutrients, infections to toxic burden and everything in between can throw a proverbial spanner in the works.
THYRO
Let’s take a look at some of the essential nutrients required to make, release and receive thyroid hormone (T4 & T3) - the THYRO part of our trio.

If any of these are missing it will result in disruption to not only the thyroid, but of course impact the entire operating system as well: HPA-O-T (hypothalamic-pituitary-adrenal-ovary-thyroid axis).
✅ Iron - needed for normal functioning thyroid peroxidase -the enzyme involved in making thyroid hormones
✅ Zinc - When levels are low, TSH is not created, resulting in low levels of thyroid hormones T4 and T3. Zinc is also an essential part of the enzyme deiodinase, which converts T4 into active T3
✅ Iodine - essential for thyroid hormone (TH) synthesis, but must exist in a narrow range It’s a delicate balance here:
⬇️ In Iodine deficiency - TSH goes up to encourage expression of the sodium / Iodide symporter (a little shuttle bus that brings iodine into thyroid gland) > the higher the TSH = a greater production of hydrogen peroxidase and oxidative damage to the thyroid
⬆️ With iodine excess, a goiter can occur due to failure to escape from the Wolff−Chaikoff effect which inhibits thyroid hormone synthesis, or due to persistent stimulation by thyroid-stimulating antibodies that keep the NIS shuttle bus activated resulting in a rush of white blood cells into thyroid and an increase in thyroid size.
✅ Selenium - required for conversion T4-T3, and as a component of the antioxidant defence Glutathione peroxidase within the thyroid itself.
✅ Mercury accumulation in the body has been shown to be highest in the thyroid & pituitary. Mercury co-accumulates with Selenium in a 1:1 ratio to protect cells against the harmful effects of Hg
✅ Vitamin A - is required for optimal thyroid receptor binding and immune modulation away from autoimmunity
✅ Vitamin D - good evidence has demonstrated an association between low vitamin D status and autoimmune thyroid diseases such as Hashimoto’s thyroiditis.
BOLIC
The bolic component of Thyro-BOLIC-pause refers to metabolic syndrome / insulin resistance & it could be occurring in your case or the driver to symptoms such as weight gain, cravings, fatigue & more.

Metabolic syndrome is a cluster of conditions, increasing your risk of heart disease, stroke & type 2 diabetes. These conditions include increased blood pressure, high blood sugar, excess body fat around the waist & abnormal cholesterol / triglyceride levels. Metabolic syndrome is also closely linked to a condition called insulin resistance.
What’s this now I hear you say? Normally, your digestive system breaks down foods into sugar. Insulin is a hormone that ushers this sugar into your cells to be used as fuel. In insulin resistance, cells don't respond normally to insulin & sugar can't enter the cells as easily, it’s like the doors get slammed shut. As a result, your blood sugar levels rise, even as your body churns out more & more insulin to try to lower your blood sugar.
So now we have a horrid situation of ❶ high blood sugars & ❷ high insulin, resulting in excess sugars being converted into triglycerides. As insulin is a storage hormone it signals for the newly formed triglycerides to be stored into adipose tissue (fat cells) specifically around the waistline & major abdominal organs, like the liver! Enter the expanding waistline & trajectory to fatty liver. To compound the issue this extra fat, especially types that accumulate in the belly area, are notorious producers of inflammatory chemicals.
So, we now know that Triglycerides are stored “energy” (unused calories essentially), which should in normal physiology be able to be accessed & released back into the bloodstream to provide the body with energy (fuel) & thus trigger weight loss. BUT in a picture of continual high insulin these triglycerides just get locked into fat cells and the signal to free them can’t get through. This constant state of inflammation inhibits your body’s ability to communicate with insulin receptors, further contributing to your body’s state of resistance, fatigue & cravings - so the vicious cycle starts again!

Some vitally important nutrients required to halt / reverse insulin resistance are:
① Omega 3 - works by reducing those pro-inflammatory chemicals that occur in the storage process of insulin resistance. Some of the main offenders being MCP-1, TNF-a, IL-6 and IL-1. Omega 3 also has an insulin sensitising effect lowering post-meal spikes in blood sugars, and improving inability to effectively use insulin.
② Alpha Lipoic Acid - works by activating a master enzyme called AMPK which is a major regulator of cellular energy metabolism - basically, it’s like putting on a pair of jump leads onto your cells!
③ Cinnamon - The results of a study by the American Diabetes Association demonstrated that intake of 1, 3, or 6 g of cinnamon per day (1 g of ground cinnamon is about half a teaspoon) reduces serum glucose, triglyceride, LDL cholesterol, and total cholesterol in people with type 2 diabetes and suggests that the inclusion of cinnamon in the diet of people with type 2 diabetes will reduce risk factors associated with diabetes and cardiovascular diseases. Add this powerhouse of a spice into your coffee, smoothie or breakfast bowl with gusto!
PAUSE
The transition into perimenopause triggers a number of symptoms: Gaining extra pounds irrespective of what you eat, anxiety. migraines, changes in periods, heavy periods, low Mood and sleep disturbances.
Many women are confused by the terminology, when asked about their menopausal status, most say that they are “in menopause” without knowing there is even a specific stage, how long it will last & what to expect.
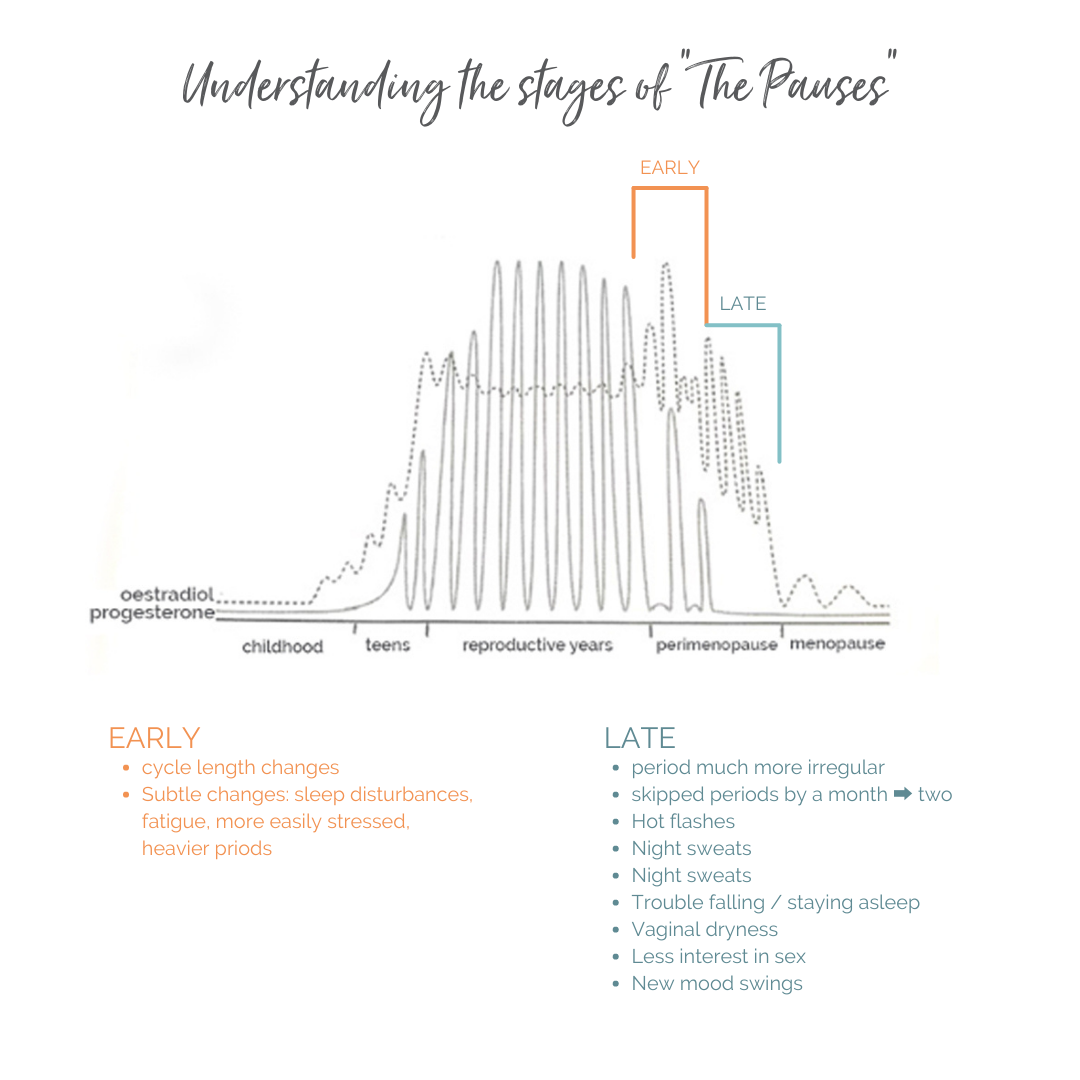
Understanding the stages of “The Pauses” that finally arrive at The Menopause helps to remove the mystery surrounding this pivotal phase of a woman’s life & importantly allows for more targeted interventions. The levels of hormones change vastly across these phases & as such require a more delicate approach vs a one size fits all - your “menopausal - HRT is the magic bullet” approach.
Perimenopause (PM) is the transition to menopause - it is just that, a slow, subtle change. It is not a night and day event. We don’t just wake up one morning, menopausal! In PM oestrogen remains high & quite erratic in nature, while progesterone plummets dramatically by comparison.
During early PM, you will notice changes in the length of your menstrual cycle of more than 7 days. Early PM symptoms are subtle for most women, often put down to “stress” not realising they’ve started the menopause transition.
Later phase of PM, signs become much more clear eg. you’ll start skipping periods, have hot flashes and other signs like trouble falling asleep. Once in late PM, the best estimate is that you will reach menopause in 1-3 years. The perimenopause is the 2-12 years before menopause.
A significant part of the transition pause is addressing this now erratic unopposed oestrogen picture (as progesterone takes a nosedive). More on this tomorrow. Together with ensuring other hormones that working in concert with sex hormones are “balanced: thyroid, cortisol & insulin levels. Stabilising these and menopause transition is an easier ride - there will still be ups and downs, BUT not so much of a rollercoaster ride. Many if not most of perimenopausal symptoms stem largely from losing progesterone, leaving an unopposed and erratic oestrogen.

Nutrients for support:
Nutrient ① Magnesium. As cited in this review: The Effects of Magnesium Supplementation on Subjective Anxiety and Stress—A Systematic Review: Magnesium may modulate anxiety by increasing GABA - which is the brain’s main calming or inhibitory neurotransmitter.
Nutrient ② Taurine - Is another calming neurotransmitter like GABA . By “tickling” GABA receptors, taurine works really nicely with magnesium to support “GABAergic” activity, which helps to improve sleep, which can help to prevent migraines. Taurine also improves healthy insulin sensitivity (see last week's post) through quashing reactive oxygen species (ROS) insulin resistance causes.
Nutrient ③ B vitamins. The role of compounds from the group of vitamin B cannot be overestimated in the perimenopause and menopause. Folate and vitamins B2, B6 and B12 are all essential in the life-force process of methylation and plays an important role in maintaining the functions of the nervous system. Deficiencies in any of these B vitamins will disrupt detoxification, mood, energy delivery, immunity and cognitive function.
Nutrient ④ Quercetin - Reduces histamine and mast cell activation. Oestrogen increases histamine which is a stimulating neurotransmitter that can cause anxiety, insomnia, fluid retention, headaches or migraines.